Erectile Dysfunction: The Canary in the Cardiovascular Coal Mine?
The role of endothelial function on tumescence – and beyond
By Erica Zelfand, ND
The stories I hear of men* with erectile dysfunction (ED) are strikingly similar: The issue begins insidiously and is initially treated at a “low T clinic” with gradually increasing doses of exogenous testosterone in regimens that yield varied but ultimately insufficient results.
A review of the lab work of these individuals reveals that they are typically overdosed on their prescription hormones, with total testosterone levels often above 1000 ng/dL. While supraphysiological levels of testosterone do, in fact, enhance the sexual desire and performance of some men, they come with significant health risks and pesky side effects like anxiety, irritability, and insomnia. Other men, however, find that even high doses of anabolic steroids fail to engender desired outcomes in the bedroom.
Erectile dysfunction (ED, impotence) is a fairly common medical condition, characterized by the inability to achieve and maintain a penile erection firm enough for satisfying sexual intercourse.1 ED is also on the rise: While the condition affected an estimated 152 million males worldwide in 1995, that number is expected to swell (no pun intended) to over 320 million people by 2025.2,3
Just last week, a new patient shouted at his wit’s end, “I’m taking testosterone, HCG [human chorionic gonadotropin], and anastrozole. I’m lifting more weight than the other guys at the gym. I look amazing. I have tons of energy—so much I can’t fall asleep at night – but I after two years of playing with all my doses I still can’t get hard. What the heck is wrong with me!? What are my other doctors missing? I really hope you can figure it out.” [Note: This patient employed more expletives when expressing himself.]
Time and time again, I explain to exasperated fellows like this one that sex hormone levels are just one piece of the puzzle. The successful treatment of ED often also entails assessing the nervous system (including mental health), adrenal function, metabolic health, and endothelial integrity, with the latter being among the most overlooked aspects of sexual health.
Tumescence is a hemodynamic process characterized by enhanced penile arterial inflow and reduced venous outflow.4,5 Because the physiology of tumescence (penile erection) requires that the penis engorges with blood, the integrity of the vascular system—and ergo the status of nitric oxide production—is of utmost importance to male sexual performance and satisfaction.6
Nitric Oxide: The Endothelium Relaxer
Our understanding of nitric oxide (NO) is relatively new: In 1998 three American pharmacologists received the Nobel Prize for their discovery of NO’s effects as a signaling molecule within the cardiovascular system.7
This tiny gas molecule is produced in the blood vessels, nerves, and immune cells. Neuronal and endothelial NO causes relaxation of the surrounding smooth muscle, resulting in vasodilation.8,9 With regard to male sexual health, NO triggers the relaxation of the cavernous smooth muscle of the penis, allowing for engorgement and subsequent erection.
NO production declines with age, however, placing males at increased risk of ED as they grow older.10 It is now estimated that nearly half of men above the age of 40 have some degree of ED.11
Endothelial inflammation undermines NO production and is thus a significant determinant of ED and other vascular diseases.12 It is also a culprit that can effectively be treated with naturopathic medicine.
Erectile Dysfunction as Coronary Risk Marker
Due to the relatively small size of the penile vasculature (on even the most well-endowed of individuals), ED may be understood as a warning sign of poor vascular function and impending coronary artery disease (CAD).9,11,13,14 ED may present well before the observation of so much as an elevated blood pressure reading.15 If left unchecked, the vascular inflammation and dysfunction associated with many cases of ED may lead to ischemic heart disease;16 ED has thus been referred to as “penile angina.”17
ED is such a strong predictor of cardiovascular disease in men,3 in fact, that providers are now advised to assess the cardiovascular health of patients presenting with the condition.16 While not all men with ED have cardiovascular problems, a significant percentage of males with angiographically demonstrated CAD have been observed to have ED.13 ED was also shown in one study to precede CAD in a whopping 70% of male CAD patients.13
It is perhaps no surprise that ED and CAD go hand-in-hand, as they share many of the same risk factors, including sedentary lifestyle, obesity, diabetes, smoking, hypertension, dyslipidemia, metabolic syndrome, and declining NO activity.9,11,18,19
Conventional Treatments of ED
The first-line therapy for ED entails phosphodiesterase type 5 inhibitors (PDE5i) like sildenafil.20 Although these drugs do not directly increase NO, they do augment NO-mediated pathways.21
When PDE5i’s fail to improve symptoms, vacuum devices, intracavernous injections, and penile prosthesis implantation are considered second- and third-line therapies. Few patients are eager to try these interventions, however, which may not be too great of a tragedy, as none of these methods adequately addresses the underlying metabolic, neurological, hormonal, or endothelial aspects of ED.
Testosterone plays an important role in sexual function via several mechanisms, including the stimulation of NO release.22 As more and more males become afflicted with ED, the increasing number of “low T” clinics that have cropped up over the years now comprise a multi-billion-dollar industry.23,24 Testosterone replacement therapy (TRT) does help many men with ED—though not all. In my experience and opinion, focusing on NO augmentation—either in lieu of or in addition to hormone prescription—may serve ED patients in both the short and long term.
Erectile Dysfunction: The Canary in the Cardiovascular Coal Mine?
Two Pathways of Nitric Oxide Production
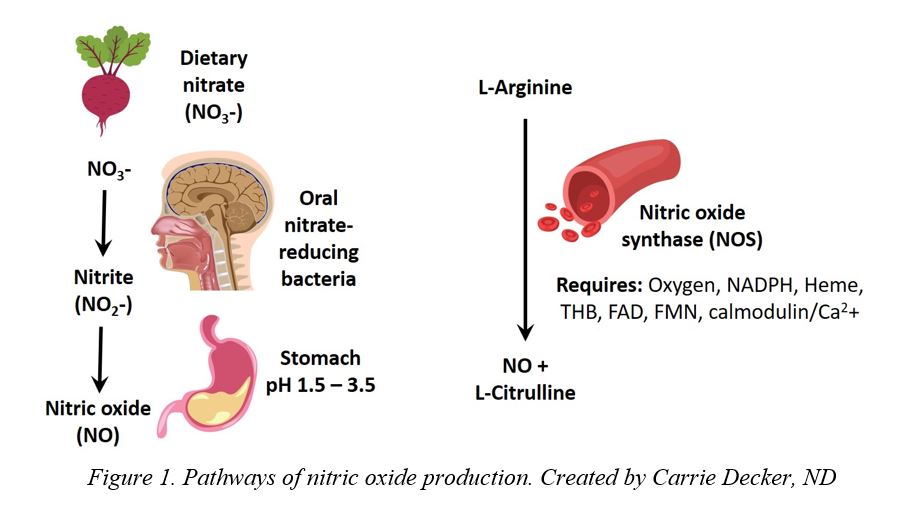
There are two pathways by which NO is created in the body (see Figure 1).25 One pathway entails the reduction of dietary nitrates to nitrite and then NO.26 Another pathway depends upon the enzyme nitric oxide synthase (NOS) to convert L-arginine to NO.27
Oral Hygiene
In the NOS independent pathway of NO production, facultative oral microflora reduce dietary nitrates (NO3–) to nitrites (NO2–), which are then converted to NO in the acidic environment of the stomach.26
In this pathway, the presence of particular oral bacteria and the stomach’s low pH are invaluable for NO production. These requisite conditions are undermined, however, by antiseptic mouthwashes, proton-pump inhibitors, and over-the-counter antacid medications—agents commonly used in industrialized societies.28–30 Although restoring a patient’s gastric acidity is a relatively straightforward task for the naturopathic physician, as of this writing there is no nutritional probiotic supplement that contains the oral bacteria essential for nitrate reduction. We may still, however, advise patients to avoid commercial mouthwash products.26
Dark Leafy Greens and Beetroot
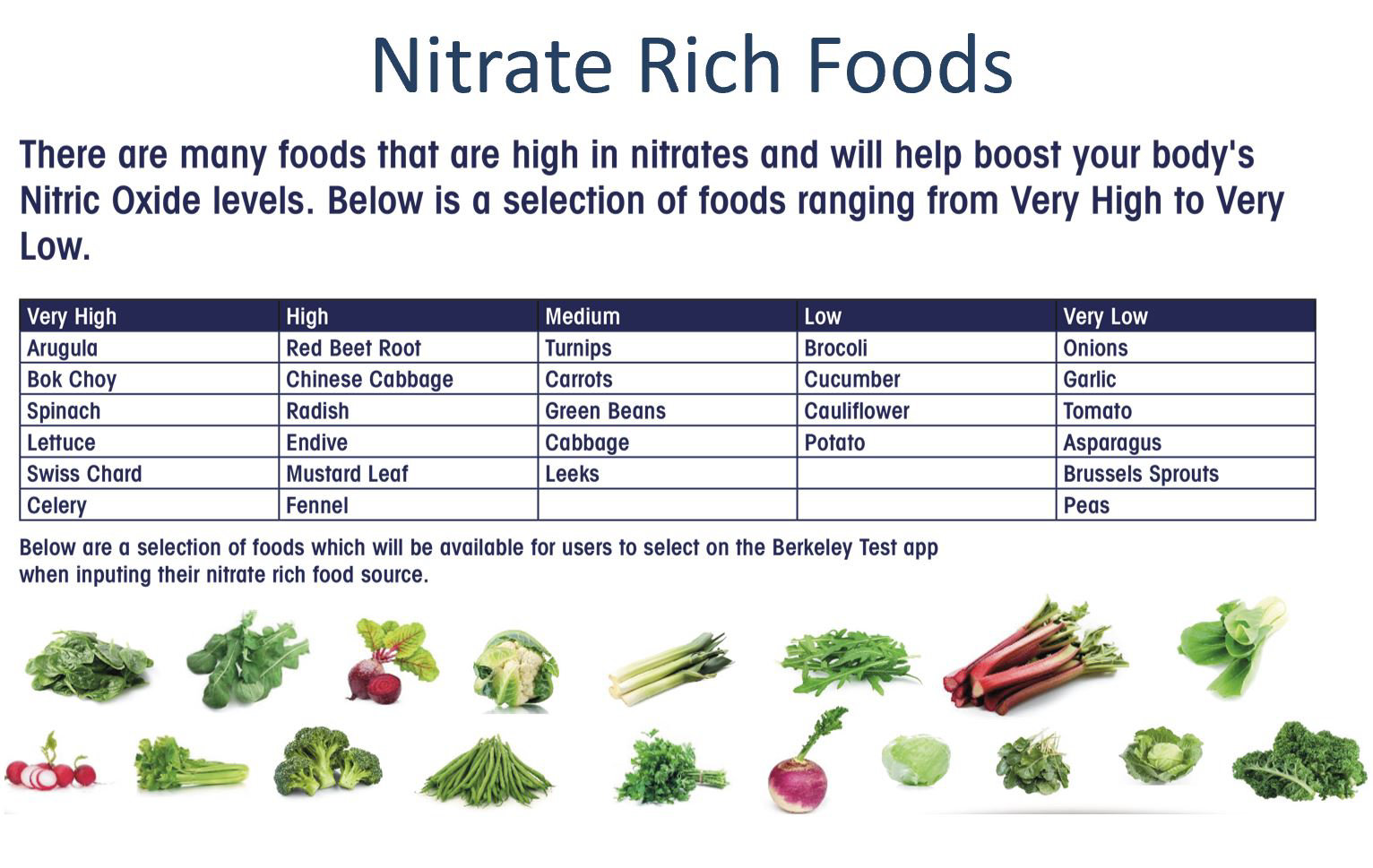
Vegetable-rich diets have been shown to support heart health,31,32 in part due to their nitrite and nitrate content. High nitrate diets lower the risks of hypertension, heart attack, and stroke,33–35
Although dietary nitrites such as those naturally found in bacon have been vilified, nitrites and nitrates are actually naturally occurring molecules produced in the body that are important to health.36,37 (The culprit in processed meats is likely not nitrite, but rather the carcinogenic compound nitrosamine.38,39)
In addition to eating plenty of green, leafy vegetables, powdered greens products, beetroot (also known simply as “beets”), and beetroot products may all be used as supplemental sources of nitrates, antioxidants, and phenolic compounds pertinent to cardiovascular health.40 Beetroot is a particularly rich source of nitrates and antioxidant compounds and has been observed to increase NO levels and lower blood pressure readings in both men and women of various ages.41–43
Although dietary nitrites such as those naturally found in bacon have been vilified, nitrites and nitrates are actually naturally occurring molecules produced in the body that are important to health.36,37 (The culprit in processed meats is likely not nitrite, but rather the carcinogenic compound nitrosamine.38,39)
In addition to eating plenty of green, leafy vegetables, powdered greens products, beetroot (also known simply as “beets”), and beetroot products may all be used as supplemental sources of nitrates, antioxidants, and phenolic compounds pertinent to cardiovascular health.40 Beetroot is a particularly rich source of nitrates and antioxidant compounds and has been observed to increase NO levels and lower blood pressure readings in both men and women of various ages.41–43
L-Arginine and L-Citrulline
L-Arginine may be acquired from nutritional supplements and/or endogenously derived from the amino acid L-citrulline, and serves as the source raw material from which the body produces NO via NOS (Figure 1).44 Low serum levels of L-arginine have unsurprisingly been correlated with poor NO production.45
A significant percentage of ED patients have low L-arginine or L-citrulline levels, placing them at increased risk of disease.45 Because of this and because the NOS-dependent route of NO production was the first pathway discovered, the nutraceutical product market is now replete with L-arginine-containing formulae.46
Although oral L-arginine supplementation may improve NO-mediated vasodilation and endothelial function, its effects as a monotherapy are transient due to the short duration of its presence in the circulation (on the order of milliseconds).47 This may be why a review of L-arginines efficacy in the treatment of ED reports that a minimum dosage of 3 g daily is necessary to achieve outcomes. Some studies have even dosed the amino acid at 5 g and higher.48
The efficacy of L-arginine may be improved by delivering it alongside N-acetylcysteine or glutathione (GSH), both of which contain sulfur residues or thiols. NO binds GSH, forming S-nitrosoglutathione. This molecule then transports and circulates NO, has a half-life of hours, and is just as vasoactive as NO.49 Antioxidants like ascorbate also are able to cleave or release bound NO.50 L-arginine also pairs particularly well with Pycnogenol, as is explored in the section below.
Unlike L-arginine, its precursor L-citrulline (named for the watermelon, or Citrullus vulgaris, from which it is derived51) evades presystemic metabolism, effectively increasing circulating NO levels.45,52,53 This may make L-citrulline a more advantageous nutritional supplement than L-arginine in the treatment of ED, hypertension, and related vascular conditions.54,55
Although L-citrulline supplements are less effective than PDE5i’s (at least in the short term), they are an effective adjuvant to PDE5i treatment.54,56 L-citrulline has also been shown to be safe and psychologically well tolerated.54
What may be even more effective than L-arginine or L-citrulline monotherapy, however, is the administration of the two NOS substrates concurrently: Simultaneous oral supplementation of L-arginine and L-citrulline (1 gram of each) increased plasma L-arginine levels more than 2 g of either alone in a 2017 study.57 (Note that because many viruses, including herpes simplex virus [HSV], are dependent upon the bioavailability of arginine,58 L-arginine and L-citrulline supplements may be poorly tolerated by patients with frequent HSV outbreaks.)
In addition to augmenting the body’s supply of L-arginine, it is also important to support conversion of the amino acid into NO.38 This conversion is enhanced by oxygen, NADPH, heme, tetrahydrobiopterin (THB, also known as BH4), and other coenzymes. Things as simple as checking oxygen saturation and ferritin levels may therefore prove advantageous.
Pycnogenol
A standardized extract from the bark of the French maritime pine, Pinus pinaster—or Pycnogenol, as it’s known in the US by its patent name—can improve erectile function both as a stand-alone treatment and in combination with L-arginine.59,60
In a double-blind study of 21 males suffering from ED, patients received 120 mg of Pycnogenol or placebo daily. After three months, Pycnogenol significantly improved the symptoms of ED from moderate to mild stage. Perhaps more importantly, a significant increase in plasma antioxidant activity was noted among those who received Pycnogenol, while no such benefit was found in those who received placebo. The Pycnogenol group further enjoyed reductions in total cholesterol and LDL-cholesterol levels (from 5.41 to 4.98 mmol/L and from 3.44 to 2.78 mmol/L, respectively). (No significant changes in triglycerides or HDL were observed.) These findings suggest that Pycnogenol may not only treat ED but may also temper some of the more serious vascular changes that succeed it.61
In another study of 40 males, 25 to 45 years of age, a combination of L-arginine and Pycnogenol significantly outperformed Pycnogenol alone, helping 80% of men (and, after another month of the study, 92.5% of men) achieve a normal erection – as compared to only 5% of men who benefitted from Pycnogenol alone. Pycnogenol was given at a dose of 40 mg one to three times daily, with L-arginine at a dose of 1.7 g daily.60 (It is worth noting that the minimum effective daily dosage of L-arginine as a standalone treatment of ED may be 3 g,62 though this study suggests that lower doses may be used within the milieu of co-treatment with Pycnogeol.)
In a similar trial of 50 males, L-arginine (3 g/day) plus Pycnogenol (80 mg/day) restored normal erectile function after just one month of supplementation. Sperm quality improved in the men who took this combination and their testosterone levels increased significantly. The men also reported a doubling in their sexual intercourse frequency.63
Glutathione and Other Antioxidants
Supplementation with L-citrulline and GSH has also been shown to synergistically increase NO levels.
In addition to providing thiols for the formation of S-nitroso glutathione, GSH also affects the NOS enzyme function. In a GSH-depleted environment, NOS becomes uncoupled, resulting in the production of toxic superoxides instead of salubrious NO. Endothelial NOS (eNOS) uncoupling has been implicated in numerous conditions marked by vascular endothelial dysfunction, including heart failure, ischemia/reperfusion injury, hypertension, atherosclerosis, and diabetes.65
As the master antioxidant of the body, GSH strongly protects against the oxidative stress associated with endothelial dysfunction. Like other antioxidants, GSH may prevent eNOS uncoupling by scavenging free radicals, mitigating certain radical-generating pathways, maintaining the optimal ratio of reduced to oxidized glutathione, and protecting the endothelium against damage by toxic metabolites.66
GSH and other antioxidants can thus prevent oxidative stress, ameliorate vascular endothelial dysfunction, and stave off cardiovascular disease (among other chronic ailments).66
DHEA
The steroid hormone precursor dehydroepiandrosterone (DHEA) not only augments hormone production, but also positively affects eNOS. Supplementation with DHEA may thus further support endothelial health.67 A systematic review of 38 trials found that DHEA improves various aspects of sexual health in both males and females, including sexual interest, sexual frequency, lubrication, arousal, pain, and orgasm.68
Carnitine and Taurine
Carnitine and taurine have been shown to support NO production and vascular health. Specifically, propionyl-L-carnitine (PLC) has been observed to stimulate NO production and facilitate the delivery of free fatty acids into the mitochondria.69 When administered alongside acetyl-L-carnitine, PLC enhances the efficacy of sildenafil in treating the symptoms of ED in men who have undergone bilateral nerve-sparing prostatectomy.70
Taurine also increases NO, likely by decreasing asymmetric dimethylarginine (ADMA), as an inhibitor of NO synthesis.71,72
Meditation
Beyond erectile function and blood pressure, NO’s benefits include blood clot prevention, immune function enhancement, and nervous system support.7 NO may also contribute to the relaxing effects of meditation and mindfulness practice—and mindfulness practice may likewise enhance NO production.73 In one study, for example, experienced meditators were found to have lower levels of subjective stress and higher nitrate and nitrite levels.9 This finding may be added to the long list of reasons to recommend meditation and other mindfulness-based practices to those with ED and other cardiovascular ailments.
Exercise
Sedentary lifestyle is a significant risk factor for both ED and cardiovascular disease.9 Physical activity is known to increase vascular NO levels and improve vascular function,74 which explains at least in part why exercise is hailed as the lifestyle factor most strongly correlated with erectile health.74,75
A 2018 systematic review of 10 studies concludes that moderate to vigorous aerobic exercise four times weekly for six months improves erectile function in men who have ED caused by sedentary lifestyle, obesity, hypertension, cardiovascular disease, and/or metabolic syndrome.9 Considering that exercise helps with a wide array of other health conditions, physical activity should be a basic treatment guideline for just about every patient.
Conclusion
During sexual arousal, the vessels of the penis rely upon nitric oxide to help blood—and the oxygen and nutrients it carries—engorge the penis, resulting in tumescence. Erectile dysfunction may therefore represent poor endothelial health and a deficit of NO in many cases—and thus serve as a warning sign of more serious vascular ailments to come.
Because there is no standard lab test for assessing NO levels,76 it is important for healthcare providers to make astute clinical assessments of their patients’ cardiovascular status when labs and imaging fall short.
Simple, natural strategies and supplements—like oral health, digestive hygiene, green vegetables and beetroot, L-arginine, L-citrulline, glutathione, DHEA, carnitine, Pycnogenol, meditation, and exercise—may well serve the men who suffer from erectile dysfunction. Even in the context of testosterone replacement and phosphodiesterase inhibitor prescription, nitric oxide support may further improve sexual performance and safeguard against more serious vascular disease.
- L-Arginine and L-Citrulline
- Pycnogenol
- Glutathione and Other Antioxidants
- Carnitine and Taurine
- __Berkeley Life Pro, __ M3 Powder, __ NO Max ER
- Testosterone __ IM, __Troche,__ Topical
- DHEA
- Meditation
- Exercise